
Structural Defects Of Enamel
Introduction
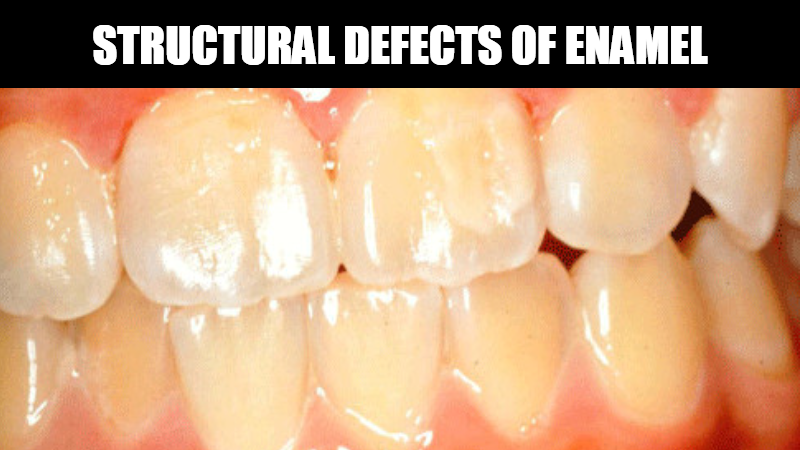
Enamel is unique in that remodeling does not occur after initial formation. Therefore abnormalities in enamel formation are etched permanently on the tooth surface. The timing of ameloblastic damage has a great impact on the location & appearance of the defect in the enamel.
Classifications
- According to Shafers, Naville:
Two basic types of enamel hypoplasia are –
1. Hereditary type – Amelogenesis imperfecta
2. Type – Environmental Factors
· Nutritional deficiency ( Vitamin A, D & calcium)
· Exanthematous diseases
· Congenital syphilis
· Birth injuries
· Local infection/trauma
· Ingestion – chemicals
· Fetal alcohol syndrome & cytotoxic chemotherapy.
According to Roderick, A Cawson:
1. Defects of enamel :
– Ameligenesis imperfecta
a. Hypoplastic
b. Hypocalcified
c. Hypomaturation
– Defects of dentin:
a. Dentinogenesis imperfecta
b. Shell teeth
c. Dentinal dysplasia
d. Regional odontodysplasia (Ghost teeth)
2. Multi-system Genetic Disorders with Dental Defects :
· Osteogenesis imperfecta
· Ehlers – danlos syndrome
· Hypoparathyroidism
· Epidermolysis bullosa
· Cleidocranial dysplasia
3. Acquired (mainly metabolic) disorders:
· Flurosis (mottled enamel)
· Celiac disease
· Rickets (Dietary and renal)
· Syphilis
· Childhood fevers (linear defects)
· Turner’s tooth
· Fetal alcohol syndrome
· Cytotoxic chemotherapy
CAUSES OF ENAMEL HYPOPLASIA
Local causes
· Infection
· Trauma
· Irradiation
Generalized causes
· Genetic : Amelogenesis Imperfecta
· Environmental
Prenatal –
· Rubella
· Syphilis
· Flouride ions
· Maternal diseases
Neonatal –
· Hypocalcaemia
· Prolonged labor
· Premature birth
Postnatal–
· Measles
· Chickenpox
· Scarlet fever
· Pneumonia
· Hypoparathyroidism
· Fluoride ions
· Cancer chemotherapy
Environmental enamel hypoplasia:
1. Mild type:
Maybe only a few small grooves, pits, or fissures on the enamel surface.
2. Severe type:
May exhibit rows of deep pits arranged horizontally across the surface of the tooth. A considerable portion of enamel may be absent. Suggesting prolonged disturbance in the function of the ameloblasts.
| Environmental type | Hereditary type |
| Either deciduous or permanent dentition is affected. | Both the dentition is affected. |
| Affect both types of hard tissues. | Either enamel or dentin is affected. |
Environmental Enamel Hypoplasia in Detail
- Nutritional deficiency (Vitamin A, D & calcium)
- Vitamin A deficiency.
- Rickets :
- Rickets – In children.
- Osteomalacia – In adults.
Teeth appear to have some priority over the skeleton when the supply of minerals is inadequate. Dental defects have been described only in exceptionally severe cases of dietary rickets. Dental defects of rickets comprise defective calcification of the enamel and dentin with a wide zone of predentin and large amounts of interglobular dentine.
In severe cases, the eruption of teeth is delayed. Rickets during the time of tooth formation is the most common cause of enamel hypoplasia.
Hypocalcemia: Pitting variety of enamel hypoplasia is seen. Maybe caused due to:
- Tetany due to decreased level of calcium.
- Vitamin D deficiency.
- Parathyroid deficiency.
Hypoplasia Due To Exanthematous Fevers
Exanthematous Fevers including Measles, Chickenpox & Scarlet fever are etiologic factors that occur during the first 2 years of life, also called “Chronological hypoplasia”.
A common pattern: linear defects typically consist of a groove or line of pits across the labial surface of the enamel, usually near the junction of the incisal third and cervical 2/3rd. The enamel loss is bilaterally symmetric and the location of the defects correlates well with the developmental stage of the affected teeth. Most cases of enamel hypoplasia involve those teeth that form within the first year after birth. Thus the teeth most frequently involved are the central and lateral incisors, cuspids, and first molars.
Enamel Hypoplasiaue to Congenital Syphilis
This hypoplasia involves the maxillary and mandibular permanent incisors and the first molars. Anterior teeth affected are called“ Hutchinson’s teeth ” while the molars have been referred to as Mulberry Molars(Moon’s Molars, Fourniers molars).
The upper central incisor is Screw driver shaped, the mesial and distal surfaces of the crown tapering and converging toward the incisal edge of the tooth rather than toward the cervical margin. The incisal edge usually has crescentic notches or fissures. Although the maxillary lateral incisor is normal. The cause of tapering & notching has been explained on the basis of an absence of the central tubercle/calcification center.
The Pathogenesis of these defects is speculative, but Treponema Pallidum has been demonstrated within the developing dental follicle. It has been suggested that chronic inflammation & fibrosis compress the developing tooth and that folding of the ameloblast layer causes characteristic notching / other deformities.
Hypoplasia Due to Birth Injuries
The Neonatal line/ring that can be seen microscopically in non-decalcified ground sections of deciduous teeth & 1st permanent molars can be considered a mild form of enamel hypoplasia, a disturbance indicative of the trauma or change of environment at the time of birth.
In traumatic births, the formation of enamel may even cease at this time. Enamel hypoplasia is far more common in prematurely born children than in normal-term infants.
In most cases, enamel hypoplasia of deciduous teeth enamel formed after birth is involved.
Enamel Hypoplasia due to Infection/Trauma
A type of hypoplasia in that only a single tooth is involved, most commonly one of the permanent maxillary incisors / maxillary or mandibular premolars
There may be a degree of hypoplasia, ranging from mild, brownish discoloration to severe pitting & irregularity of the tooth. These single teeth are referred to as Turner’s Teeth and the condition is called Turner’s Hypoplasia. The incisal 3rd most severely affected.
If a deciduous tooth becomes carious during the period when the crown of the succeeding permanent tooth is being formed, a bacterial infection involving the periapical tissue of this deciduous tooth may disturb the ameloblastic layer of the permanent tooth and result in a hypoplastic crown. A similar type of hypoplasia may follow trauma to a deciduous tooth, particularly when the deciduous tooth has been driven into the alveolus and has disturbed the permanent tooth bud. If the permanent tooth crown is still being formed, the resulting injury may be manifested as a yellowish or brownish stain or pigmentation of the enamel, usually on the labial surface, or as a true hypoplastic pitting defect or deformity.
Enamel Hypoplasia due to Fluoride
A well-recognized example of chemically induced generalized enamel hypoplasia results from the ingestion of fluoride.
Fluoride-induced enamel hypoplasia is usually inconspicuous at levels below 1.0 ppm in drinking water. With increased amounts of fluorides in the drinking water, the resultant enamel hypoplasia becomes progressively evident.
Pathogenesis:
Increased fluoride levels interfere with ameloblastic function, which adversely affects both enamel matrix formation & matrix calcification. Deciduous teeth are rarely affected.
Clinical features:
Depending upon the Level of Fluoride in the water supply, there is a wide range of severity in the appearance of mottled teeth varying from
- Minimal / Questionable
- Mottling exhibits a smooth enamel surface with occasional subtle whitish flecking.
- < 25% of the tooth surface is involved.
- 0.5 – 1.5 ppm.
- Mild
- Exhibits smooth surface with opaque white areas.
- 50% of the tooth surface is involved.
- 2.5 ppm.
- Moderately to Severe
- Exhibits varying degrees of obvious pitting with paper white or brownish discoloration
- The whole enamel surface is involved.
- 4.5 ppm.
- Severe
- The enamel is considerably softer & weaker than normal with widespread pitting defects & brownish discoloration, resulting in excessive wear and fracturing of the incisal and occlusal surfaces.
- 6.0 ppm & more.
Foetal Alcohol Syndrome:
Excessive consumption of alcohol during pregnancy may lead to a facially & mentally abnormal foetus. Dental development may be delayed and there may be enamel defects such as mottled opacities near incisal margins & elsewhere, abnormally translucent enamel.
Hypoplasia due to Antineoplastic Therapy / Cytotoxic Chemotherapy
Children surviving malignant disease particularly acute leukaemia, may have dental defects as a result of chemotherapy. Teeth may have short roots(radicular hypoplasia), and hypoplasia of enamel. Microscopically prominent incremental lines corresponding with the timing of the chemotherapy. In extreme cases, teeth may fail to develop.
Radiation therapy can be responsible for most severe developmental alterations; the most severe alterations are associated with radiation doses as low as 0.72Gy and are associated with mild defects in both enamel & dentin. Frequently noted alterations include hypodontia, microdontia, radicular hypoplasia, and enamel hypoplasia.
Developmental Disturbances in the Structure of Enamel
Amelogenesis Imperfecta:
It is a heterogeneous group of hereditary disorders of enamel formation affecting both primary & permanent dentitions. These disorders are confined to the enamel.
Depending on the clinical presentation of the defects and the likely stage of enamel formation that is primarily affected,
May be classified into:
- Hypoplastic
- Hypocalcified
- Hypomaturation
- Both with Taurodontism
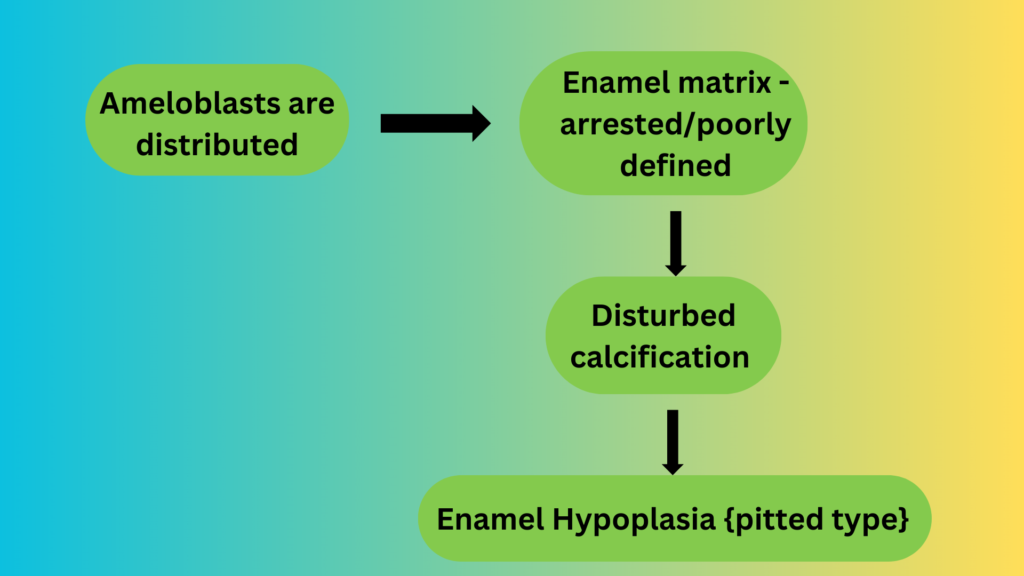
Hypoplastic AI:
Exhibits decreased enamel matrix formation caused by a disturbance in the functioning of the ameloblasts. Any matrix present is mineralized appropriately and radiographically contrasts well with the underlying dentin.
Depending upon the mode of inheritance & clinical appearance the defective Enamel may be sub-classified as:
- Generalized pitted :
Pinpoint to pinhead-sized pits are scattered across the surface of the teeth and do not correlate with a pattern of environmental damage. Buccal surfaces of teeth are severely affected and pits may be arranged in rows/columns & staining of pits may occur. Enamel between the pits is of normal thickness, hardness & coloration.
- Localized Pattern:
Shows horizontal rows of pits, linear depression, or one large area of hypoplastic enamel surrounded by a zone of hypo calcification typically located in the middle 3rd of the buccal surfaces of the teeth. The incisal or occlusal surface is not affected.
Both dentitions, All teeth / only scattered teeth. Autosomal recessive is more severe and typically demonstrates the involvement of all teeth in both dentitions.
Autosomal Dominant Smooth Pattern:
Enamel of all teeth exhibits a smooth surface & is thin, hard & glossy. Appear like Crown preparations and demonstrate open contact points because of the absence of appropriate enamel thickness. The color is opaque white to translucent brown
Radiographically exhibit a thin peripheral outline of radio-opaque enamel.
X – Linked Dominant Smooth Pattern:
Males with X- linked dominant smooth pattern exhibit diffuse thin, smooth & shiny enamel in both dentitions. Appear like crown preparations with open contact points. Color ranges from brown to yellow-brown.
Females exhibit vertical furrows/ridges of thin hypoplastic enamel, alternating bands of the normal thickness of enamel.
Rough Pattern
Enamel is thin, hard & rough surfaced. Teeth taper towards incisal/occlusal surface and demonstrate open contact points. Enamel is denser than the smooth pattern. The color is white to yellow-white. A radiographically thin peripheral outline of radiodense enamel is seen.
Enamel Agenesis:
Demonstrates a total lack of enamel formation. The color is yellow to brown hue. Open contact points and crowns taper towards the incisal/occlusal surface. The surface of dentin is rough. Anterior open bite. Radiographically no peripheral enamel overlying dentin. Lack of eruption because of no significant resorption.
Hypomaturation Amelogenesis Imperfecta:
The Enamel matrix is laid down appropriately and begins to mineralize but there is a defect in the maturation of the enamel’s crystal structure. Normal in shape but exhibit a mottled, opaque white brown yellow discoloration. Enamel is softer than normal and tends to chip from the underlying dentin.
Radiographically enamel exhibits a radiodensity that is similar to dentin.
Pigmented pattern:
The surface enamel is mottled & agar brown. Often fractures from the underlying dentin &
soft enough to be punctured by a dental explorer. Often demonstrates extensive calculus deposition.
X- Linked Pattern:
Males
Exhibit different patterns in primary and permanent dentitions. Deciduous show opaque white to translucent mottling. Permanent teeth show opaque yellow white & darken with age. Enamel tends to chip & degree of enamel loss is rapid. Radiographically contrast between enamel & dentin is reduced
Females
Similar patterns are seen in both dentitions. Vertical bands of white opaque enamel & normal translucent enamel. Bands are random & asymmetric. Transillumination is often required to demonstrate this pattern.
Snow Capped Pattern:
Exhibit a zone of white opaque enamel on the incisal/occlusal ¼th of the crown. Demonstrate an X- linked pattern of inheritance. Often demonstrate anterior to post distribution and have been compared with a denture dipped in white paint. Both dentitions affected
Hypocalcified Amelogenesis Imperfecta:
Enamel is very soft & easily lost. On eruption, the enamel color ranges from yellow to brown / orange later stained brown to black. Exhibits rapid calculus apposition. Loss of coronal enamel except in the cervical Portion.
Hypomaturation / Hypoplastic AI – Taurodontism:
Both dentitions are affected. The two patterns are similar but differentiated by the thickness of enamel & overall tooth size.
Hypomaturation – Hypoplastic pattern:
Predominantly hypomaturation in which enamel appears mottled yellowish white to yellowish brown. Pits are seen frequently on the buccal surfaces of teeth. Radiographically enamel appears similar to dentin in density and large pulp chambers in addition to varying degrees of taurodontism.
Hypoplastic – Hypomaturation pattern:
The predominant defect is hypoplasia in which enamel is thin & demonstrates hypomaturation. R/G is similar to the hypomaturation / hypoplastic variant except for a decrease in the thickness of enamel. Both patterns are seen in Trichodento-Osseous Syndrome.
Trichodento- Osseous Syndrome
Autosomal dominant syndrome. Systemic changes like kinky hair, osteosclerosis, and brittle nails are seen. If only dental changes are seen in the absence of hair / bony changes then AI is appropriate.



Very valuable info